A pancreatic pseudocyst is a circumscribed
collection of fluid rich in pancreatic enzymes, blood and necrotic tissue,
typically located in the lesser sac of the abdomen. It is normally a
complication of pancreatitis, although in children pancreatic pseudocysts often
occur following abdominal trauma.
 They account for approximately 75% of all the
pancreatic masses.
They account for approximately 75% of all the
pancreatic masses.
Nevertheless, our patient was never
diagnosed with pancreatitis before, but for about 6 weeks he had complained of
strong epigastric pain (not acidic in nature), not responding to any treatment
for peptic ulcer disease.
He came to our observation because of an
extremely tender epigastric mass. He was actually referred from another
facility with diagnosis of perforated duodenal ulcer.
We immediately performed an abdominal ultrasound
which allowed us to exclude any viscus perforation or peritonitis. On the other
hand we have actually seen a round mass of the epigastrium, measuring about 12
cm in diameter. The mass was clearly a cyst, but the content was thick and rich
in debris; it was clearly outside the liver parenchyma, and so it could not be
an amoebic liver abscess.
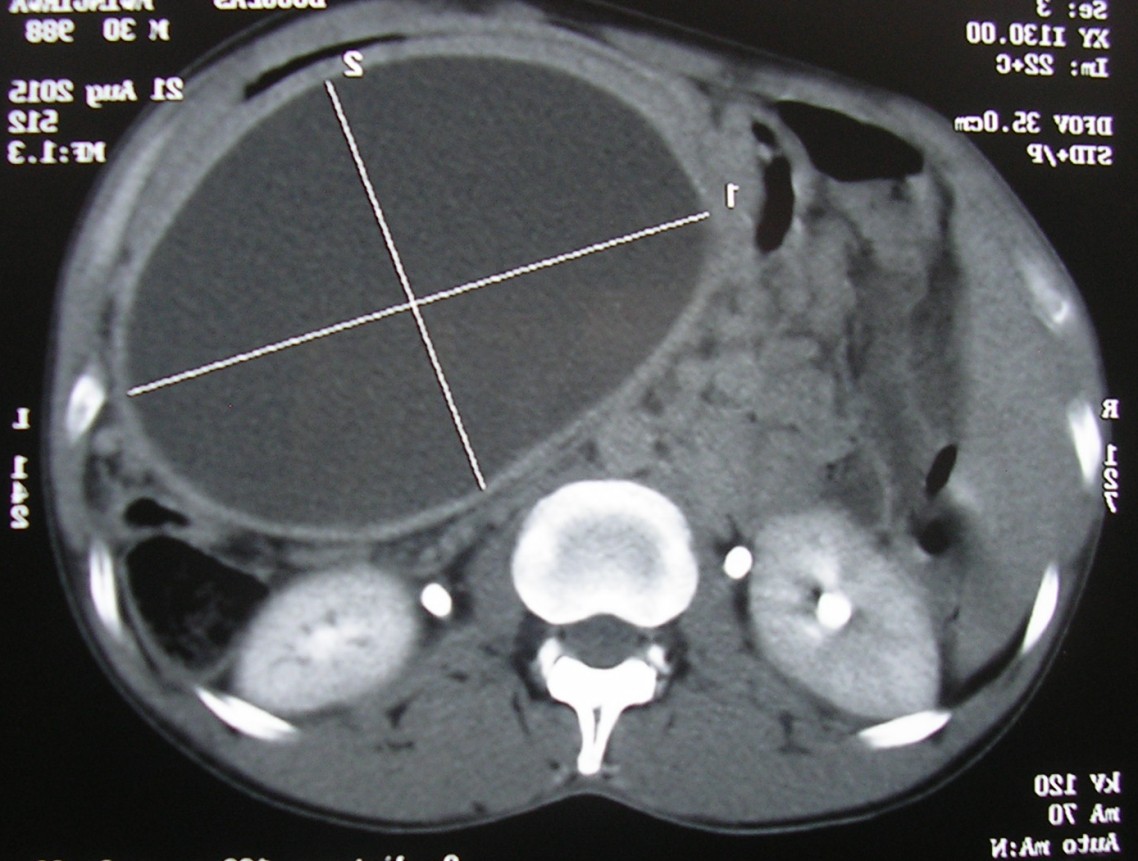
Because of the epigastric location, immediately
I have thought of a possible pancreatic pseudocyst, but I have decided to
confirm the diagnosis with an abdominal CT scan. The latter imaging test was
completely in accordance with the finding of the ultrasound, and I was a bit
proud of that.
The patient was always in great pain and he
demanded a solution to his problem.
We have studied; we have consulted our
mentors, and finally we have decided that the only way to help him was through surgery.
We went to theater the following day. The
patient was intubated and given general anaesthesia.
We have then opened the abdomen with a
midline xyfo-umbilical incision, which has given us a good view of the
epigastrium and of the stomach in particular.
The pancreatic pseudocyst was behind the
stomach itself and it was completely attached to it: that was good news from
the surgical point of view.
We have opened the anterior wall of the
stomach; thereafter we have operated a small incision through the posterior
wall of the stomach and the attached cyst: through the opening, we have sucked
around 250 ml of brownish fluid, paying a lot of attention to avoid any spill
in the peritoneal cavity… we actually feared a possible chemical peritonitis
caused by the high concentration of pancreatic enzymes in the cystic material.
We have then made a continuous hemostatic
suture on the posterior wall opening, and eventually we have closed the anterior
wall of the stomach in two layers.
In such a way we have created a continuous
drainage of pancreatic juice in the stomach itself. Before closing the abdomen
in layers, we have abundantly washed the peritoneal cavity with warm saline
solution.
The patient is now doing well in his
post-op recovery and we have high hopes he will completely recover.
Dr Bro Giuseppe Gaido

Nessun commento:
Posta un commento